In recent weeks Londonwide LMCs has been receiving increasing reports from practices about a sharp rise in FP69 flags and high numbers of patient deductions by PCSE. In some cases, practices report hundreds of FP69 flags being set at once, representing between 1% and 10% of their patient list.
Practices are concerned about:
- adverse impact on patient care,
- the impact on financial viability,
- the lack of time to put mitigations in place,
- the volume of FP69s,
- the number of inappropriate deductions,
- the subsequent list size reductions, the shorter timeframe for them to validate those deductions with PCSE, and
- the volume of workload created.
This financial and operational impact is most acutely felt by practices with deprived populations, while the lack of predictability makes it difficult for practices to do any proper financial and business planning.
This guidance outlines what we know of the PCSE list validation process and provides routine proactive measures practices can put in place to maintain their list, as well as practical steps before, during and after PCSE exercises to mitigate their impact.
We are currently trying to build a picture of how significant the impact of this change is on practices and patients across London. It would help us in our influencing work if you could take five minutes to fill in this form about how your practice has been affected.
Following widespread concerns raised by the profession, Londonwide LMCs has submitted an FOI to NHS England to establish the assessed impact and scope of the process on practices.
NHS England wrote to practices on 10 July 2026, setting out why they feel the process is justified and proportionate. The letter does not make any commitments to alter the list cleanse process as currently being implemented.
Patient communication resources
We have produced some wording to share with patients, available as a poster (PDF or Jpeg), a video clip and text to paste into WhatsApp. Due to the nature of FP69 flags, for patient communications to be effective practices need to encourage people who do currently engage with contacts to cascade the information to friends, family, housemates, etc who are registered by not engaging with the practice. See more in the proactive messaging section.
{kind=link}
Text to paste into WhatsApp
*What is a “ghost patient”?*
👻 A “ghost patient” is someone who remains on the practice list despite having moved away or otherwise no longer being an active patient.
*What you need to know – NHS list validation*
📋 You may receive a letter from NHS England or Primary Care Support England (PCSE). This is part of a routine process called list validation (or list cleansing). It helps ensure GP records are accurate across England.
*Why this matters to you*
Keeping a patient list correct helps GPs to ensure:
🩺 You stay registered and can see your GP when you need to.
💌 You get important letters, including for screening, vaccinations etc.
💷 The practice gets the right funding to care for their patients.
*What you need to do*
📨 If you or someone you care for gets a letter, text or other message from NHS/PCSE, please respond. Do NOT ignore it.
✅ Follow the instructions in the letter.
✅ Confirm your details are correct.
✅ Reply within the deadline set out or contact your practice. The deadline may vary depending on how you are contacted by NHS/PCSE.
*What happens if you do not respond*
If you do not respond and PCSE cannot confirm your details:
⚠️ They may remove you from your practice without you even knowing it.
⚠️ If you get removed, you will not be able to get an appointment with your GP until you re-register.
*Need help?*
📱 Contact your practice via your usual preferred means.
📢 If you have friends or relatives who are patients, but have not contacted their practice in the last three years please encourage them to get in touch to update or confirm their details.
Representation approach
- We have asked LMC representatives to reach out to their practices to gather data on the extent of the problem and for practices to feed back directly via this form.
- We will be utilising this data to discuss with regional teams and ICBs any mitigations that can be put in place to prevent financial de-stabilisation of practices. This data and local insight will also strengthen our advocacy messaging.
- We have complemented your individual responses with a data dashboard which pulls together publicly available figures to show the rate of patient de-registrations across different areas of London.
Advocacy approach
- We are supporting practices to raise concerns directly and indirectly; amplifying concerns about the impact on practices and patients of current GP list cleansing activity in London across. So far we have written to:
- Decision makers – including Ben Coleman MP and Danny Beales MP who are the two London MPs on Parliament’s Health and Social Care Select Committee. We also supported LMCs in the most effected constituencies with drafting letters to their MPs.
- Influential bodies – including more than a dozen charities, patient groups and third-sector organisations.
- We have spoken to GP specialist media, including provided them with examples of practices affect, and secured coverage in the Independent, using Londonwide LMCs compiled data and LMC members as interviewees.
- If you would like to write to your MP you can use these template letters, with ICB specific figures depending on where your practice is based:
We will raise concerns about the negative impact on patients and practices of the current aggressive list cleansing programme, covering: practice stability/ revenue; health inequalities; increasing lack of access for overly-affected groups; delivery of Government health shifts regarding community care and prevention/ early treatment.
GP list validation (also known as ”list cleansing” or “list maintenance”) is the process of PCSE checking a GP practice’s registered patient list to remove perceived “ghost patients”, i.e. people who are still recorded as registered with the practice, but who have moved away, died, registered elsewhere, or are otherwise no longer genuinely patients of the practice.
Having clean practice lists means that:
- Patients remain linked to the correct practice .
- Screening and vaccination programmes reach the right people, enhancing health prevention and population coverage .
- Patients receive appropriate chronic disease management and clinical follow-up .
- Appropriate use of public funds with practices receiving the correct funding for their registered population, i.e. they are not under- or over-funded, as allocations are made on a capitation (i.e. on a £ per patient) basis.
- Practices are in a better position to achieve QOF and other performance targets and clinical outcomes as their denominators are not artificially inflated because of ghost patients .
Schedule 3, Part 2 of the GMS Regulations 2015 sets out practices’ obligations regarding maintaining accurate patient lists.
Although the GMS contract contains no single standalone clause stating this duty, Schedule 3 as a whole — covering registration, patient removals at the patient’s request or after registration elsewhere, death, moves, and absence from the UK for more than three months — sets out the practice’s obligation to take the necessary steps to maintain an accurate patient list.
NHS England has a national contract with PCSE, which amongst other responsibilities includes carrying out periodic data quality checks and reconciliations against practice lists.
PCSE manages this process on a 3-year continuous rolling programme meaning roughly a third of practices in England are contacted each year for checks on their patient list. In some cases PCSE also contact a patient directly, setting out a response window of 10 days in their letter. Patients directed to the list cleanse online form are given 30 days to update their details. We do not know what determines whether PCSE contacts a patient directly or whether they ask the registered practice to do so. Patients who have received a letter can update or confirm their address via this PCSE form, which they have 30 days from re of the letter
According to BMA practice list validation guidance, this rolling programme focuses on six main patient categories:
- Patients aged over 100.
- Patients who migrated to England one year ago (“transient” registrations) .
- Students registered at an educational establishment for four or more years .
- Children under 16 recorded as sole occupiers of a property (“orphans”) .
- Patients registered at demolished properties .
- Addresses with unusually high occupancy (8+ patients).
There is no further information available on the methodology used, the role of automated tools in identifying patients, nor a health impact assessment. PCSE state that they may contact either the practice or the patient directly to confirm their address and registration details. We are currently uncertain whether PCSE are routinely sending physical letters to patients or not.
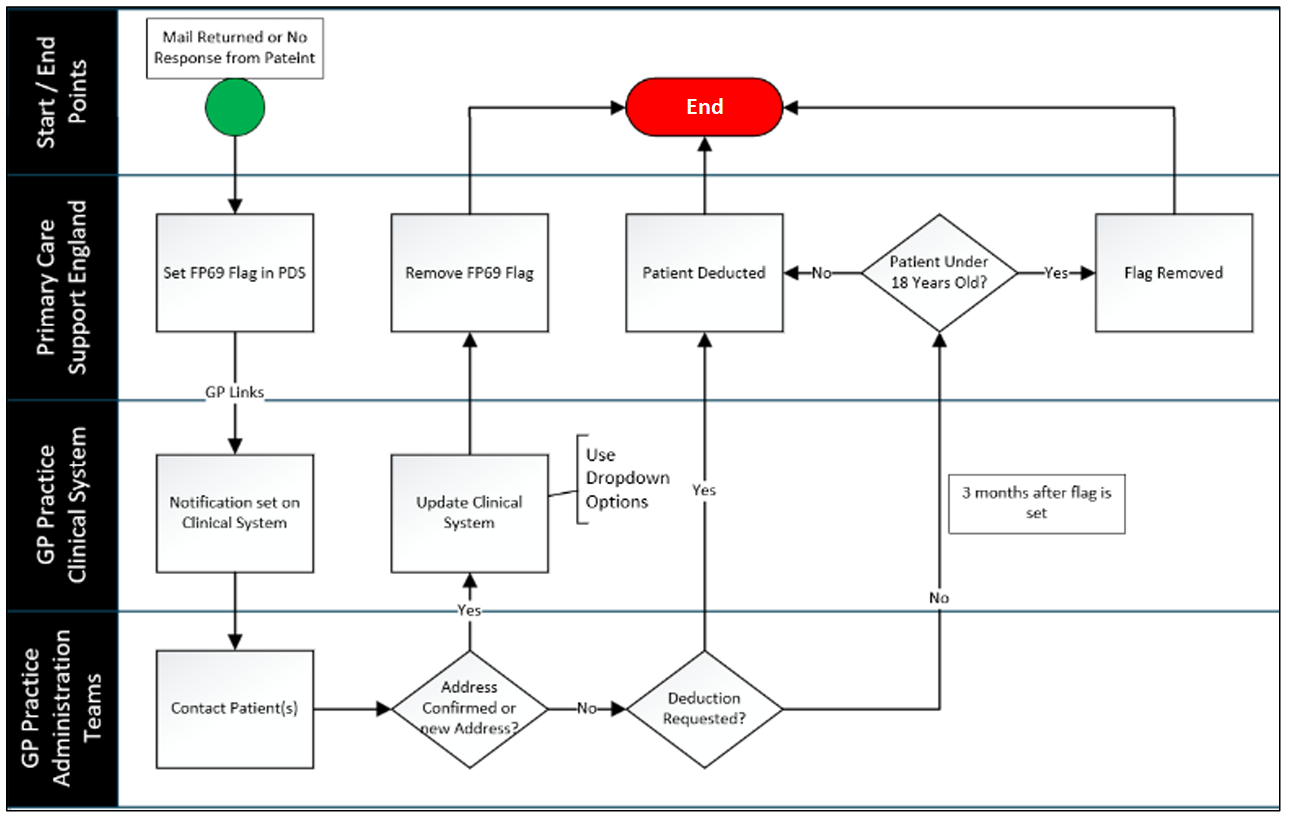
Upon the return of information, PCSE will either:
- add a note to the patient record to say that the details are correct, for example ‘reg confirmed’, ‘whereabouts known’, ‘seen recently’,
- process the patient deduction sent via GP links, or
- apply a FP69 marker or flag (which will result in the patient deducted in 3 months’ time unless an update to the patient details or a new registration is received in that time).
FP69s are flags set on patients’ Personal Demographic Service (PDS) record, when PCSE receive notification that mail to a patient has been returned undelivered, for example in response to a screening invitation letter, or as described above when a patient has failed to respond to a request to confirm their details as part of a list validation exercise.
When such a notification is received by PCSE, a FP69 flag is set on the patient’s record and the registered practice’s clinical system is notified via GP Links on the date the flag is set.
Up until 1 October 2025 practices had six months from the date the FP69 was set to accept deductions through FP69s or get the flags removed. With the new contract changes that were introduced from 1st October 2025, this window has been halved to 3 months. This is a major tightening as it means that practices must act more quickly when FP69 flags appear on their system or risk losing patients from their list along with the associated funding.
This change was communicated by PCSE to practices in their July 2025 bulletin.
On receipt of a FP69 flag, the practice has three months to contact the patient directly and confirm that:
- they still reside at their registered address, or
- they have moved address but remain in the practice’s catchment area, or
- they have moved outside the practice area but wish to remain registered and the practice is able to accommodate this, or
- according to their clinical system, the patient has been seen at the practice in the last 6 months, or after the FP69 was set but within the 3-month window.
The practice will then update their clinical system and notify PCSE accordingly via GP Links. In all those cases, the FP69 flag will be removed from the patient’s record, and the patient will not be deducted from the practice’s list.
If PCSE does not receive confirmation of any of the above within 3 months of the FP69 flag being set, the patient will be removed from the practice’s list if they are over 18. If they are under 18, they will remain registered for safeguarding reasons, but address checks still need to be carried out.
The process is described in the PCSE FAQs.
Below is a diagram showing the FP69 process:
Patients who do not respond to PCSE letters (including those who are vulnerable, elderly, have unstable/temporary housing, do not speak English etc) or those whom the practice is unable to contact and confirm their details, will be removed from the practice’s list without the patient necessarily knowing it.
Being removed means a patient would need to re-register to access GP services, which can cause a gap in care, disruption to ongoing treatment, and loss of continuity with their GP. Patients will not be contacted for screening, vaccinations, chronic disease management, or other important information about their care.
Patients in at-risk cohorts for example students, over-100s, those in houses of multiple occupancy, are most likely to be flagged.
The new shorter three-month timeframe (from October 2025) means less time for practices to catch up with FP69 flags and correct errors before a patient removal is actioned by PCSE.
- Avoid FP69 flags piling up by having systems in place to check your clinical system and “de-ghost” your list regularly (see: BMA guidance on FP69 searches).
- Allocate dedicated admin team members to monitor FP69 flags on a daily or weekly basis depending on your staff capacity.
- Keep on top of your GP Links FP69 flags and patients who the practice would be expected to deregister proactively, such as those who have died.
- It is NHS England policy that practices should remove patients who have notified you they are outside of the UK for more than 3 months.
- Run searches on patients who have not been in contact with the practice for 3 years or more and contact them proactively to check if they are still at their registered address. then note on their record that this contact has taken place. See proactive messaging section below.
- Remind patients to notify you when they have moved address or if they have changed their mobile number, so you can update their record promptly.
- Specialist practices with particularly high patient turnover (e.g. university practices) need to be even more diligent in processing patient removals for their student population at the end of each academic year.
 There may be a variety of reasons why patients do not respond to PCSE letters, such as vulnerability, old age, dementia, moving house frequently, not having English as their first language etc. Practices tell us that often their elderly patients think that such letters are scams, so they prefer not to respond to them.
There may be a variety of reasons why patients do not respond to PCSE letters, such as vulnerability, old age, dementia, moving house frequently, not having English as their first language etc. Practices tell us that often their elderly patients think that such letters are scams, so they prefer not to respond to them.
- When communicating it is worth remembering that patients you are in frequent contact with are unlikely to get an FP69 flag, but they can be a useful way of getting the news out to patients who want to remain registered with the practice but are not being reached by direct contact. For example, parents encouraging adult children to remain registered, a person telling other people in their houseshare or somebody translating the information for someone with limited English.
- To help you encourage your patients to respond to PCSE letters and practice communications, we have drafted a patient-facing poster for you to put up in your waiting area and an animation to publish on your practice website. The animation could also be shared on messaging apps and social media, if so, think about what accompanying text might be applicable to the patient cohorts you are trying to reach.
- Provide the poster to be displayed at your local school(s), community centres, places of worship and other places people meet. Particular consideration should be given to places providing services to vulnerable patients such as shelters and refuges.
- Liaise with your local pharmacist to convey message to patients – they could also display the poster in their pharmacy.
- Inform your PPG that PCSE is undertaking those checks and share the poster and animation for them to cascade to other patients they may know locally
- Add a message to patient scripts.
- Bulk text message to patients who have not been in contact for over three years.
- Familiarise yourself with the PCSE FAQs.
- Familiarise yourself with the these parts of the in the NHS England Primary Care Policy and Guidance Manual (PGM), version 6:
Do not ignore them!
- Respond promptly to any FP69 flags set by PCSE following the process outlined in this guidance and in the PCSE and NHSE links provided
Review the patient record first
- Check last consultation/contact (appointments, prescriptions, results, admin contacts).
- Look for recent activity not immediately obvious (e.g. hospital letters, online consultations, medication requests).
- Confirm whether the patient is in a care home, housebound, or receiving community care, which may explain lack of visits to the practice.
- If the patient has been ‘Recently seen’ (within the last 6 months) you can request the removal of the flag.
- If the patient has not been seen in the last 6 months, move to the following:
Check validity of patient’s details
- Confirm the patient address on your clinical system against the information held on the NHS Spine for any discrepancies.
- Look for indicators the patient may have moved (returned practice mail, no response to imms invite from the practice etc.).
- Check with known contacts or carers if appropriate.
Contact the patient
- Email and or text – quick and commonly used first step.
- Phone call(s) – try calling at different times of the day if possible.
- Send letter to the registered address if no response electronically.
- Consider contacting a cohabiting relative where other forms of communication do not reach a patient.
Follow up non-responders
- If no response is received after the initial contact, usually two to three weeks is considered reasonable to make another contact attempt.
- Record dates, methods, and outcomes of each contact attempt.
As advised by PCSE, respond to active FP69s using the available dropdowns in GP Links rather than using free text responses to avoid ambiguity on the reasons why you are challenging a patient removal. Free text responses will be interpreted by PCSE staff, so best to avoid any potential misinterpretation.
If you have requested the removal of an FP69 flag but PCSE have not actioned it and you are still within the 3-month window, PCSE advises that you try to respond to the FP69 again via your clinical system. Where possible use options available from dropdown menus.
- a. “Address unchanged and/or confirmed”, remove FP69
- b. “Patient seen”, remove FP69
If it is not possible to do a further response to the FP69 flag, please email pcse.registrations-preston@nhs.net. Please include the patients details and your practice code.
If PCSE does not receive confirmation from the practice via GP links that the patient is either still at the address or at a new address within 3 months (for any raised on or after 1 October 2025) or 6 months (for any raised on or before 1 October 2025) the patient will be removed from your list. If the letter they’ve sent to the patient is returned to them marked as ‘moved abroad’ or ‘deceased’ the appropriate action would be taken to deduct the patient from PDS (Patient Demographic System).
While there is no formal post-3 month “appeal” mechanism, it may be possible for practices to challenge PCSE if they have valid reasons to believe patients have been removed incorrectly through the FP69 process.
PCSE guidance states that if a patient has been deducted because the FP69 expired after the 3-month period and you did not confirm their details with PCSE, the patient should complete the registration process.
They go on to say that if you requested the flag to be removed and this was not done, then you should re-register the patient. So even if you have taken the correct action and there was an error on their part, they still advise that the patient should be re-registered.
We believe that there is merit in challenging PCSE in the latter scenario, i.e. where you have evidence that you have confirmed the patient details and they failed to process the removal of the FP69 within the 3-month window, following the steps below:
- Submit an enquiry to PCSE via this online form.
- Mark it as: “Incorrect patient deduction – Retrospective list amendment request”.
- Provide all the relevant patient details, deduction reason, why you believe PCSE should not have actioned this patient’s removal and evidence that the patient remained eligible, including any screenshots or audit trail from your clinical system/GP links/PDS history.
- Request that the patient is reinstated on your list and that this is backdated to the original deduction date.
If you have any particular concerns about the process undertaken by PCSE, the volume of FP69s you have received, the impact on your practice please contact our GP Support Team or your local LMC. Sharing details via this form will help us to build up up a picture of what is going on across London, but you still need to contact us directly if you need support.